How to Tell If You Have Diastasis Recti: Signs, Symptoms, and What to Do Next
Apr 04, 2026
If you’ve noticed a bulge down the center of your belly, ongoing lower back pain, or a core that just doesn’t feel right after pregnancy, you may have diastasis recti. This guide covers what it is, how to check for it at home, which exercises help, and when to see a physical therapist.
Key Takeaways
- Diastasis recti (DRA) is a separation of the rectus abdominis muscles along the linea alba, most common during and after pregnancy.
- Diastasis recti is common, affecting about 60% of pregnant and postpartum women.
- Symptoms include a midline belly bulge, core weakness, lower back pain, and pelvic floor issues.
- You can perform a simple at-home self-check using your fingers.
- The right exercises, especially those for your deep core and pelvic floor, can help reduce the separation.
- Traditional crunches, sit-ups, and full planks are usually not recommended early in recovery.
- Physical therapy (PT) for diastasis recti is the gold standard of care and can be effective even years later.
- It’s almost never too late to heal. Structured rehab can make a real difference at any stage after giving birth.
What Is Diastasis Recti?
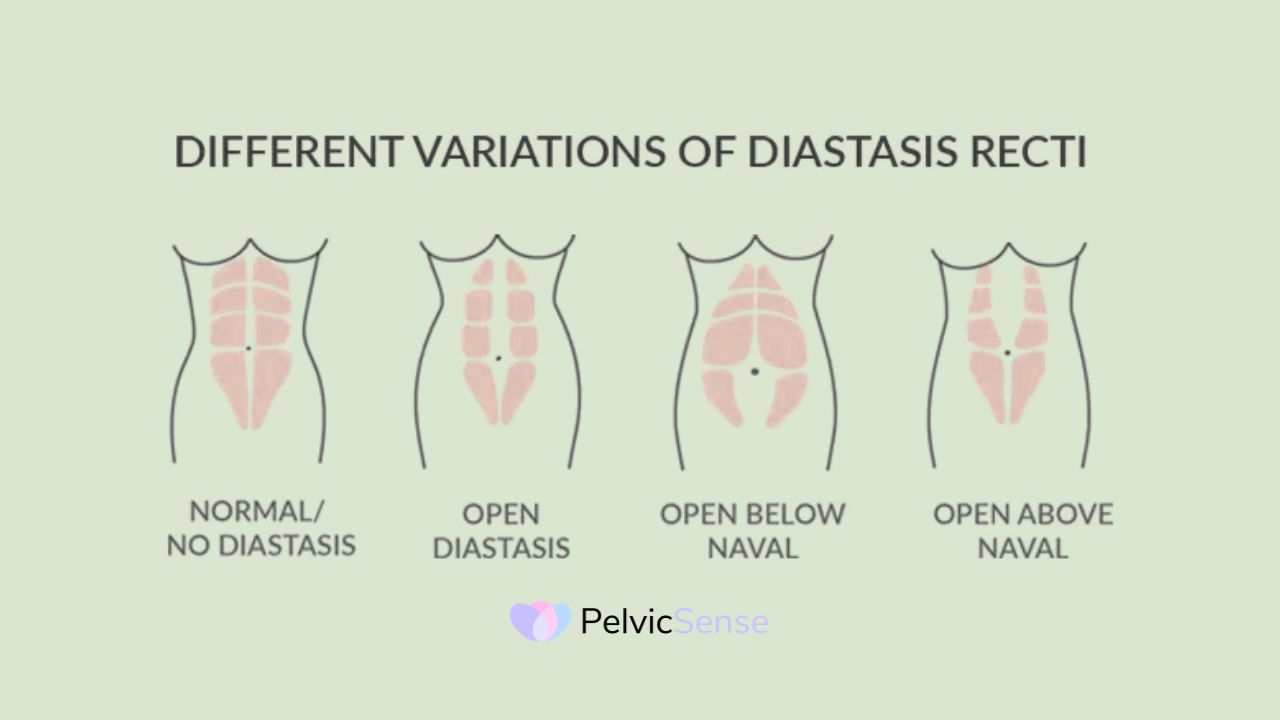
Diastasis rectus abdominis (DRA) happens when the left and right sides of your outer abdominal muscle separate because the connective tissue (called the linea alba) gets stretched too far. The two muscle bands down the center of your belly pull apart, leaving a gap held together by weakened tissue. Though often seen as a cosmetic issue, DRA has real functional effects and can affect both women and men.
The most common cause is pregnancy. As the baby grows, the uterus pushes against the abdominal wall. Combined with hormonal changes that loosen connective tissue, this creates prolonged pressure that widens the linea alba. DRA typically develops in the second or third trimester and may be noticed during or after pregnancy.
Key risk factors associated with the development of DRA include multiple pregnancies, advanced maternal age, and certain delivery methods such as cesarean sections, which may predispose the abdominal musculature to separation [4].
Diastasis Recti Symptoms You Should Not Ignore
Recognizing the warning signs is the first step to getting the right help. People with diastasis recti often tell their doctors about feeling unstable or noticing a bulge down the middle of their belly, especially when they do things that increase belly pressure, like an abdominal crunch.
Common diastasis recti symptoms include:
- A visible ridge or pooch running down the center of the abdomen
- Doming or coning of the belly when you sit up, cough, or strain
- Core weakness, which can make lifting, carrying, or keeping your body stable harder
- Lower back pain, which is a common complaint
- Pelvic floor problems, such as leaking urine or feeling pressure in your pelvis
- Abdominal pain studies consistently show women with DRA experience more belly pain than those without it, and left untreated, DRA can contribute to weakened abdominal strength, chronic lower back pain, and pelvic pain.
Symptoms vary widely. Women with DRA may have weaker abdominal muscles and more belly pain, but research shows they don’t always have more pelvic floor problems or back pain than women without it [1], which is why a professional assessment matters.
How to Tell If You Have Diastasis Recti at Home
Wondering how to know if you have diastasis recti before seeing a professional? A simple self-check can give you important clues.
Step-by-step home check:
- Lie on your back with your knees bent and feet flat on the floor.
- Place your fingertips horizontally across your midline, just above your belly button.
- Slowly lift your head and shoulders just a little off the floor, like you’re starting a crunch.
- Feel for a gap or a soft, spongy area between the muscle walls.
- Note how many fingers fit into the gap and how deep it feels.
DRA is diagnosed by measuring the distance between the two recti muscles. Abdominal palpation, tape measures, calipers, and ultrasound are the most common methods used in clinical practice.
A gap of two or more finger-widths, especially with soft tissue underneath, is worth discussing with a healthcare provider. Watch for a visible ridge or bulge along your midline when you lift your head. Remember, a home check is a starting point, not a diagnosis. Ultrasound performed by a clinician is the most accurate assessment method.
Diastasis Recti Before and After: What Changes Over Time
Diastasis recti is not permanent. Research tracking 300 women found DRA prevalence at 60% at six weeks postpartum, dropping to 32.6% by 12 months, showing that natural recovery does happen for many women [1]. However, one-third still have DRA a year after birth without treatment. A study of over 500 postpartum women found that pelvic floor strength improved and diastasis decreased with exercise [2]. If you’re wondering how to fix diastasis recti years later, recovery is still very much possible with consistent, targeted rehabilitation.
Diastasis Recti Exercises That Actually Help
Exercise is recommended as the first-line treatment for diastasis recti abdominis. But not all exercises are created equal. The goal is to build deep core stability, specifically targeting the transverse abdominis (your deepest abdominal layer) and the pelvic floor, before progressing to more demanding movements.
Research-backed exercises that support recovery include:
Diaphragmatic breathing: Learning to match your breath with core engagement is the foundation of DRA rehab.
Pelvic floor contractions (Kegels): These exercises can help close the gap in your abdominal muscles and ease pelvic pain.
Pelvic tilts: These gently activate your deep core and protect the linea alba.
Modified dead bug: Do this exercise slowly and with control, using proper breathing to avoid pressure spikes in your abdomen.
Glute bridges: These help strengthen your glutes and core, which can reduce back pain and build trunk strength.
Heel slides: This is a gentle way to work your transverse abdominis.
Modified curl-ups: Research shows these can strengthen your abdominal muscles without worsening the gap in postpartum women with diastasis recti. Broader studies also confirm that isotonic abdominal exercises, especially when paired with electrical stimulation, are among the best conservative treatments available for DRA [3].
Diastasis Recti Exercises for Recovery
A structured, progressive approach is essential. Strengthening both the abdominal and pelvic floor muscles has been shown to reduce the gap and ease pelvic pain [4]. A simple three-phase sequence works well: start with breath work and pelvic floor activation (weeks 1 to 4), progress to heel slides, glute bridges, and modified dead bugs (weeks 4 to 8), then gradually add modified curl-ups and functional movements (weeks 8 to 12+). Stop any exercise that causes doming, pain, or pelvic pressure. Aim for at least three sessions per week and allow 8 to 12 weeks before assessing your progress.
The Role of PT Diastasis Recti Treatment
Physical therapy for diastasis recti is widely recognized as the most effective non-surgical intervention. Physical therapists help adults with DRA manage their symptoms, improve their strength and stamina, and safely return to their regular activities.
The APTA Pelvic Health section has made DRA a key clinical priority, and its Journal of Women’s & Pelvic Health Physical Therapy is actively seeking new research on assessment and treatment, including exercise prescription and motor control training for postpartum women.
A pelvic health PT will:
- Measure your inter-recti distance using palpation or ultrasound.
- Assess the tension and function of the linea alba (not just the gap size).
- Evaluate pelvic floor muscle function.
- Design an individualized, progressive exercise program.
- Monitor and adjust your plan as you improve.
When booking an appointment, ask about the PT’s experience with diastasis recti and come prepared to describe your symptoms in detail.
A Smarter, At-Home Approach to Healing Diastasis Recti

Not everyone can see a PT right away, and that’s okay. Start every session with diaphragmatic breathing to manage intra-abdominal pressure. Gently engage your lower belly before any movement. If your belly domes during an exercise, the load is too much and you should regress. Strengthen your pelvic floor alongside your core, as this supports lifting, reduces incontinence, and eases pelvic pain. Progress gradually and stay consistent.
What to Avoid If You Have Diastasis Recti
Knowing what to avoid is just as important as knowing what to do. Standard crunches, sit-ups, and planks are usually not recommended for diastasis recti, especially early in recovery. Doing these moves without proper core engagement can increase pressure in your belly, which may push your organs outward through the gap or downward onto your pelvic floor.
Traditional crunches and sit-ups increase intra-abdominal pressure and can worsen separation.
Full planks: The degree of pressure exerted on the abdominal wall in a full plank creates an unsafe challenge for anyone suffering from diastasis recti.
Double leg lifts can cause or worsen abdominal separation and compromise spinal health.
Lifting with breath-holding, called the Valsalva maneuver, dramatically spikes intra-abdominal pressure.
Deep twisting movements are important to avoid, especially through the midsection, and quick twisting movements like bicycle crunches can add additional stress to the already-stretched abdominal wall.
High-impact exercise before core function is restored.
The goal is not to avoid these exercises forever, but to build a solid foundation first so you can return to them safely.
When to Seek Professional Help
While mild DRA often responds well to self-guided rehabilitation, there are clear signs that professional assessment is the right move.
See a pelvic health physical therapist or your OB/GYN if you:
- Notice a gap of more than two finger-widths that isn’t improving after 6–8 weeks of targeted exercise.
- Experience significant lower back pain, pelvic pain, or pelvic organ prolapse symptoms.
- Have urinary or bowel incontinence that isn’t improving.
- Feel a visible bulge or hernia-like protrusion at the midline.
- Are not sure whether your exercise program is helping or making things worse.
- Are more than 12 months postpartum with no measurable improvement.
In most cases, DRA improves with time and the right exercise plan. Surgery exists for severe cases that don’t respond to conservative care but is rarely the first recommendation.
FAQs
How to know if you have diastasis recti?
Use the at-home finger test described above. A gap of two or more finger-widths with soft tissue beneath is a common indicator. For a definitive diagnosis, DRA is measured by a clinician using palpation, calipers, or ultrasound. Seek assessment from a pelvic health PT or your OB for certainty.
How to fix diastasis recti years later?
Core stabilization improves function regardless of how long ago the separation occurred. A structured program of deep core and pelvic floor work can produce real improvements even years after childbirth. A pelvic health PT can design a program suited to your current level.
What exercises should I avoid with diastasis recti?
When first beginning to heal diastasis recti, you should avoid any moves that cause the abdomen to bulge or create excessive pressure, such as traditional sit-ups, crunches, v-ups, and planks. Also, avoid double leg lifts, bicycle crunches, and any heavy lifting that involves breath-holding. These movements can increase intra-abdominal pressure and widen the gap before your core has the stability to handle the load.
How do you tell if you have abdominal separation?
Look for a visible ridge or tent shape down your abdomen when you sit up, a persistent belly pooch that doesn’t respond to exercise, core instability during everyday activities like lifting, or lower back and pelvic discomfort. The separation often shows as a bulge along the midline during movement.
When is it too late to heal diastasis recti?
There is no hard cutoff. Many women resolve DRA naturally in the first postpartum year, but for those with persistent separation, structured rehabilitation has been shown to reduce the gap and improve function even years later. Start an individualized program rather than waiting.
Final Thoughts
Diastasis recti is more common than most people think, and far more treatable than many fear. Whether you are six weeks or several years postpartum, the steps are the same: understand your condition, choose the right exercises, avoid movements that make things worse, and don’t hesitate to reach out to a pelvic health physical therapist. The APTA Pelvic Health section continues to strengthen the evidence base for DRA assessment and management, which means the tools and guidance available to both clinicians and patients keep getting better. Your core supported you through pregnancy. Now it’s time to support it back.
References
- Sperstad JB, Tennfjord MK, Hilde G, Ellström-Engh M, Bø K. “Diastasis recti abdominis during pregnancy and 12 months after childbirth: prevalence, risk factors and report of lumbopelvic pain.” *British Journal of Sports Medicine*. 2016;50(17):1092–1096. https://bjsm.bmj.com/content/50/17/1092
- Bigdeli N, Yalfani A, Doosti-Irani A, Qodrati A. “An evidence-based comparison of rehabilitation strategies for diastasis recti abdominis in postpartum women: a systematic review and network meta-analysis.” *Scientific Reports*. 2025;15(1). https://www.nature.com/articles/s41598-025-22574-2
- de Oliveira LC, de Almeida LIM, Lucio MCF, Campos Júnior JF, de Oliveira RG. “Effects of conservative approaches for treating diastasis recti abdominis in postpartum women: A systematic review and meta-analysis.” *Medicine*. 2025;104(23):e42723. https://journals.lww.com/md-journal/fulltext/2025/06060/effects_of_conservative_approaches_for_treating.56.aspx
- Li M, Wang N, Wang R, Liang B. “Ultrasonographic evaluation of diastasis recti abdominis and its association with pelvic floor dysfunction in postpartum women: a cross-sectional study of a two-year retrospective cohort.” *Frontiers in Medicine*. 2024;11:1441127. https://www.frontiersin.org/journals/medicine/articles/10.3389/fmed.2024.1441127/full
Author
